 |


Ultrasonic examination
|
|
|
|
It is more useful nowadays. (Fig. 150)

Fig. 150. Transverse fetal lie in US.
Vaginal Examination
During pregnancy: the presenting part is so high that it cannot be identified properly but one can feel some soft parts.
During labor: an elongated bag of the membranes can be felt if it is not ruptured prematurely. Palpation of such parts as acromial process, scapula, clavicle and axilla helps identify the shoulder. The characteristic features are the feeling of the ribs and intercostal space. On occasion, the arm is found prolapsed. It should be remembered that the finding of a prolapsed arm is confined not only to transverse lie but it may also be associated with compound presentation. Rarely a leg may be prolapsed. Frequently a loop of umbilical cord may be found alongside the arm.
Clinical Course of Pregnancy and Labor
The course of pregnancy is usually normal except for high risk of premature labor.
The course of labor in transverse and oblique lying of the fetus is complicated. There are a lot of dangerous situations during labor, which lead to maternal and fetal death.
There may be premature or early rupture of the membranes with escape of good amount of liquor amnii because of absence of ball valve action of the presenting part. The hand of the corresponding shoulder may be prolapsed with or without a loop of cord. The cord may be prolapsed with intrauterine fetal death as a result. There is an increased chance of ascending infection from the lower genital tract. With increasing uterine contraction, the shoulder becomes wedged and impacted into the pelvis and the prolapsed arm becomes swollen and cyanotic. Gradually features of obstructed labor occur. The situation is called a neglected shoulder (Fig. 151), aka neglected transverse lying, persistent transverse lie. Neglected shoulder means a series of complications that may occur due to shoulder presentation when the labor is left uncared. The impacted shoulder usually results in obstructed labor, and later on in the uterine rupture with clinical evidence of shock and sepsis. Thus, the mother and the fetus are at highest risk of the perinatal and maternal mortality.
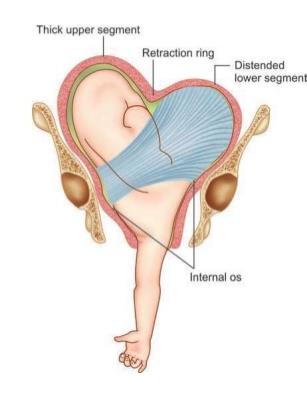
Fig. 151. A neglected shoulder
Management of pregnancy and labor in transverse lying of the fetus
The transverse (oblique) lying of the fetus diagnosed at terms of 32-34 weeks may change spontaneously to the longitudinal lie Version of the fetus can be promoted by lying on the side where a large underlying part of the fetus (head or pelvis) is found. For example, if the head is located in the left iliac region, the pregnant is recommended to sleep on her left side. The fundus of the uterus and the pelvic end of the fetus will thus be deviated to the left and the fetal head — to the right, towards the pelvic inlet. The oblique lying can be transformed into the longitudinal one. If the head is in the right iliac region, the pregnant should sleep on her right side. Sometimes malpresentations can be remedied by special exercises (alternate lying for ten minutes on the right and the left side within an hour, 3 or 4 times a day).
|
|
|
Spontaneous delivery in transverse (oblique) lying of the fetus is absolutely impossible. So, the external version of the fetus may be advised in pregnancy.
If malpresentation persists till 35th or 36th week of pregnancy, the woman should be hospitalized till delivery. The physician should attempt the external version to convert the transverse or oblique presentation into the longitudinal one, if there are no contraindications. If the pelvis of the fetus assumes a lower position on oblique presentation, the podalic version is easier to perform. The version is surprisingly easier but the chance of reversion is bigger. The version can correct only the lying, but not the reason. This demands a routine follow-up for a week after the version. If reversion occurs, such reasons as contracted pelvis, placenta praevia or congenital malformations of the fetus and uterus should be excluded, and attempt of version should be repeated. The longitudinal lying of the fetus after the version should be fixed with spindle sheets on both sides of the uterus and bandage.
If external version fails, the fetus is turned internally during labor with subsequent extraction of the fetus.
The recourse to internal version should be made with a fully dilated cervix and intact membranes (the membranes are ruptured during version), or the fetus may be versed immediately after the drainage of amniotic fluid. It is therefore very important that the membranes remain intact till the end of the first stage of labor, i. e. till the cervix is fully dilated. The parturient is prohibited to get out of bed; she is recommended to lie on that side where the fetal head (or the buttocks, if they are closer to the pelvic inlet) is found. The early loss of amniotic fluid can cause the rising infection of the uterus, prolapse of the arm, umbilical cord.
If the amniotic fluid escapes spontaneously, an immediate vaginal examination should be made to the parturient: if the cervix is fully dilated, the fetus is turned and extracted; if dilation is incomplete, cesarean section should be done. More often in modern obstetrical practice a planed cesarean section (before the onset of labor) is the only method of management of patients with transverse and oblique presentation.
In a dead or congenitally malformed fetus a destructive operation should be done. However, cesarean section is performed at availability of absolute indications to cesarean section (for example, a dead fetus, total placenta praevia).
In neglected shoulders both versions and cesarean section are contraindicated. Thus, only a destructive operation on the fetus to diminish its bulk, so as to facilitate extraction through the birth canal is indicated.
Self Test
1. Transverse lying of the fetus is the position,
A. when a long axis of the fetus lies perpendicularly to the maternal spine or centralized uterine axis.
B. when a long axis of the fetus corresponds to a long axis of mother.
C. when the fetal axis is placed obliquely to the maternal spine.
2. Spontaneous delivery through the natural ways in transverse or oblique lying of the fetus is
A. impossible
B. possible
3. The 1st position in transverse lying of the fetus is:
|
|
|
A. the head directed to the left maternal side
B. the head directed to the right maternal side
4. The 2nd position in transverse lying of the fetus is
A. the head directed to the left maternal side.
B. the head directed to the right maternal side.
5. Which of the following may lead to transverse lying of the fetus?
A. EPH-complex in pregnancy
B. placenta previa
C. post-term pregnancy
6. A preferable method of labor in transverse or oblique lying of the fetus is
A. cesarean section
B. natural ways of labor
7. The diagnostics of transverse lie of the fetus is based on
A. examination of abdominal shape
B. disparity of height of uterus and term of pregnancy
C. results of external palpation by Leopold
D. results of vaginal examination
E. all above-mentioned
8. The most common complication in transverse lie of fetus in the 1st stage of labor is
A. early rupture of bag of membranes
B. prolapse of umbilical cord
C. excessive labor pains
D. weak labor pains
E. threatened rupture of uterus
CHAPTER 19. Obstetric Versions and Extractions of the Fetus by the podalic end
Obstetric Versions
An obstetric version is an operation by which the fetus is turned into longitudinal lie for delivery.
The following obstetric versions are differentiated: external version, classical internal version with fully dilated cervix, and internal version with incomplete dilation of the cervix (Brexton-Hicks version). Brexton-Hicks version is not used in modern medicine.
External cephalic version
The external cephalic version is used in transverse or oblique lie of the fetus. Sometimes breech presentation may be another indication to external version.
The external version in transverse and oblique presentation should be performed in hospital in the 35th-36th week of pregnancy.
The conditions permitting the external version are:
· good mobility of the fetus (the amniotic fluid has not escaped);
· manageable abdominal wall;
· the uterine tonus is normal;
· normal size and architecture of the maternal pelvis;
· normal size of the fetus;
· fetus is alive;
· good health of the mother;
· pregnant agrees to the operation.
Oblique presentation can be corrected without any external manipulation: the patient is offered to lie on her side (incompliance with the position of the large presenting part of the fetus). If it fails, the fetus is turned externally.
Contraindications are:
· hemorrhages during this pregnancy;
· threatened abortion during this pregnancy;
· spontaneous abortion or premature labor in the previous history;
· hydramnios, oligohydramnios;
· multiple pregnancy;
· contracted pelvis;
· pregnancy with EPH-complex, cardiovascular diseases, etc;
· congenital anomalies of the uterus, tumors;
· adhesions in the abdominal cavity after any operations;
· the scar on the uterus after cesarean section, conservative myomectomy;
· contracted vagina (because of scars).
The fetus head is usually brought down by external version. If the head is located near the pelvic inlet, it is brought down, and vice versa, if buttocks are closer to the pelvic inlet, the fetus is turned with its podalic end toward the pelvic inlet.
The operation should be performed without anesthesia.
Technique: The patient lies in dorsal position, on a firm bed. Her bladder and rectum are empty. The woman bends her legs and the physician sits on her right side, face to face. One hand of the physician rests on the fetal head and the other one on the fetal buttocks. By careful manipulations the head is moved toward the pelvic inlet and the buttocks towards the fundus of the uterus. When the fetus is turned into the longitudinal lie, measures are taken to prevent its return to malpresentation; two pads (rolled up bed-sheets) are placed by sides of the fetus (its back and the smaller parts flexed on the chest and abdomen) and bandaged in this position without pressing tightly on the maternal abdomen (Fig. 152, 153).
|
|
|
Fig. 152. External version of the fetus.
Fig. 153. External cephalic version of the fetus: continuation.
Classic Podalic Version with a Fully Dilated Cervix (Internal Version)
Indications for podalic version are as follows:
· transverse lie of the fetus (if external version fails);
· deflexed presentation and asynclitism (brow presentation, face presentation, posterior face presentation, posterior asynclitism);
· prolapse of the umbilical cord and smaller parts of the fetus in cephalic presentation;
· complications and diseases endangering the mother and fetus (premature separation of placenta, etc).
Contraindications are:
· neglected shoulders;
· threatened rupture of the uterus;
· rupture of the uterus;
· the scar on the uterus after cesarean section or conservative myomectomy;
· cephalopelvic disproportion.
The requisite conditions are the following:
· full dilation of the cervix;
· intact membranes or just escaped amniotic fluid;
· the fetus is fully mobile in the uterine cavity;
· absence of cephalopelvic disproportion (absence of pronounced contracture of the pelvis).
General anesthesia is necessary in this operation. The operation should be performed in sterile conditions.
Technique
The operation comprises the following manipulations: introduction of the operator’s hand into the uterus, identification of the leg, grasping the leg, and version proper.
A repeated external and vaginal examination is required before the operation in order to determine exactly the position and presentation of the fetus, degree of cervix dilation, and other important factors.
Introduction of the operator’s hand
Usually the right hand has to be internal, as it is more skilful. However some surgeons prefer the left hand to be internal. The rule may be used: when the fetus is to be turned from transverse lie into longitudinal one, the internal hand should correspond to the pelvic end of the fetus (left hand to the left and right hand to the right position of the fetus).
The external hand is used to open the pudendal cleft, and the internal hand shaped into a cone is introduced into the vagina and moved towards the uterine cervix (the back of the hand should face the sacrum). When the fingers reach the cervical os, the external hand should be placed on the uterine bottom. The fetal membranes are then ruptured and the hand is moved farther into the uterus (Fig. 154).

|
|
|
